Otosclerosis and Stapedectomy
What is Otosclerosis?
Otosclerosis is a genetically determined abnormality of the bones of the human ear. Throughout life all bones are continually reabsorbed and reformed. In Otosclerosis this process does not occur normally. This can result in a number of abnormalities in the ear. The most common problem is fusion of the Stapes, one of the three bones of hearing (ossicles) that connect the eardrum to the inner ear. This then results in hearing loss.
It may be unilateral or bilateral, most commonly commencing between 20 and 50 years of age and may occur with or without a family history of Otosclerosis.
Symptoms of Otosclerosis
Conductive (Middle Ear) hearing loss
This is the most common symptom of Otosclerosis. In conductive hearing loss inner ear function is normal but damage to the ossicles decreases the efficiency of sound transmission from the outside world to the inner ear. The hearing loss is normally of a mild to moderate degree.
Sensori-neural (inner ear) hearing loss
In some cases the abnormal bone metabolism can go on to affect the inner ear resulting in what is known as a sensory neural hearing loss. The inner ear or cochlea converts the mechanical energy of sound into nerve impulses. When this occurs it is an additional hearing loss on top of the already existing conductive hearing loss in most cases. As such the loss is usually more severe.
Tinnitus
Tinnitus is an abnormal perception of sound and sufferers hear a constant or pulsatile tone. It occurs in many ear conditions and is often but not always present in Otosclerosis.
Balance Disturbance
Disturbance of balance occurs in a minority of cases of Otosclerosis and is usually mild.
Treatment options
The main objective of treatment is to rehabilitate hearing as much as possible. This is particularly important in bilateral cases but unilateral hearing losses often also benefit from assistance.
Hearing aids are generally the first line treatment in mild to moderate cases. It would be unusual to proceed to surgical treatment without first trying a hearing aid.
Surgical options include;
- Stapedectomy for moderate losses
- Bone anchored hearing aids
- Cochlear implants may be necessary in severe cases
Stapedectomy
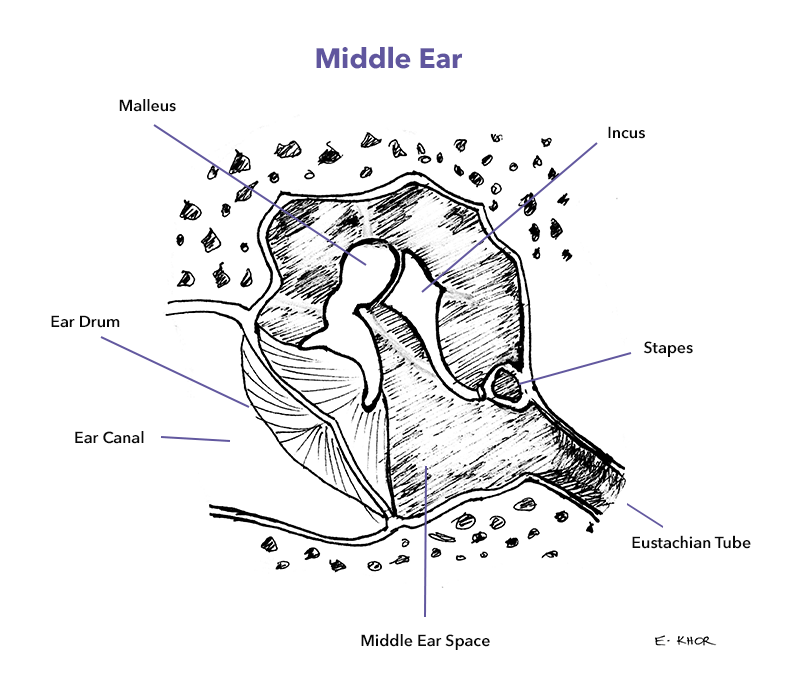
This is an operation designed to correct the most common abnormality causing hearing loss in Otosclerosis. Namely fixation of the stapes bone. The stapes is the last of the three ossicles and moves like a piston in and out of the inner ear thereby transmitting the sound waves to the inner ear.
The advantage of Stapedectomy over hearing aids is the probability restoring hearing 24 hours a day without the need for a hearing aid. Not needing a hearing aid can be especially useful at night, particularly for parents. The disadvantages are the risks discussed below
The operation

Stapedectomy is performed in hospital, usually under general anaesthesia. Most patients will stay in hospital overnight post-operatively.
A small incision is made in the ear canal. A portion of the skin of the ear canal and the eardrum are then elevated to allow access to the middle ear. In most cases a small amount of bone needs to be gently removed to allow a good view of the stapes.
The affected stapes is then partially removed and replaced with a prosthetic stapes thereby re-establishing soundwave transmission to the inner ear.
The eardrum is then returned to its normal position, the ear canal packed and the incision sutured. A dressing and head bandage are then applied.
After surgery
The first night
Like most ear operations pain is minimal. The most common issue in the early post-operative phase is dizziness, which can be quite significant but generally resolves within a few days or less.
Discharge from hospital
The morning following surgery the bandage will be removed and replaced with the smaller cotton wool dressing. Providing a normal diet is being tolerated and dizziness is absent or minimal, discharge will occur mid-morning.
Activity
For the first few weeks I prefer the avoidance of strenuous activity. The duration will depend on the individual operation but will be for at least two weeks.
Pain relief
Paracetamol or Nurofen are both fine if required, adults may take codeine containing analgesia such as panadeine if required.
Postoperative instructions
You will be given instructions for care upon discharge. These are also available to download here. At discharge you will also be given a post-operative appointment and my mobile phone number.
Risks and Complications
Success rates with Stapedectomy are high however there is a small risk of around 1% of complete hearing loss in the operated ear. If this does occur a hearing aid will no longer help and the only way to reinstate some hearing in the affected ear is a cochlear implant.
Clearly this is a bad outcome. In people considering this surgery I will always have a long discussion about the pros and cons and risks and benefits.
With Stapedectomy there is also a small risk of worsening tinnitus, balance or taste. There are also limitations on activity long-term. In particular flying in unpressurised aircraft and diving are inadvisable.